Breast Implant Illness: What Does the Evidence Actually Say?
If you have breast implants and have been experiencing unexplained fatigue, brain fog, joint pain, or other systemic symptoms — you are not imagining it, and you are not alone. Breast Implant Illness (BII) is one of the most discussed yet least formally defined topics in cosmetic surgery today. This guide explains what the current evidence shows, what we still don't know, and what your options are.
What Is Breast Implant Illness?
Breast Implant Illness (BII) is an umbrella term for a constellation of systemic symptoms that some women with breast implants attribute to their implants. Australia's Therapeutic Goods Administration (TGA) also refers to this as Systemic Symptoms associated with Breast Implants (SSBI).
Importantly, BII is not yet formally recognised as a distinct medical diagnosis with agreed diagnostic criteria. That doesn't mean the symptoms aren't real — it means the medical community is still building the evidence base needed to define and standardise it.
What makes BII complex is that its symptoms are non-specific — they overlap with many other conditions including autoimmune disorders, thyroid dysfunction, fibromyalgia, and depression. This makes it genuinely difficult to establish a direct causal relationship between the implants and the symptoms.
What Are the Symptoms of BII?
Symptoms vary widely between individuals and can affect multiple body systems simultaneously. Research shows the most commonly reported include:
According to the US Food and Drug Administration, symptoms include fatigue, memory and concentration problems, joint and muscle pain, hair loss, weight changes, anxiety, and depression — and have been reported with all types of implants regardless of filling, shape, or surface texture.
Crucially, symptoms can appear at any point after surgery — immediately, or years later. Research suggests an average onset of around 6.4 years post-implantation, though this varies considerably.
What Does the Current Evidence Say?
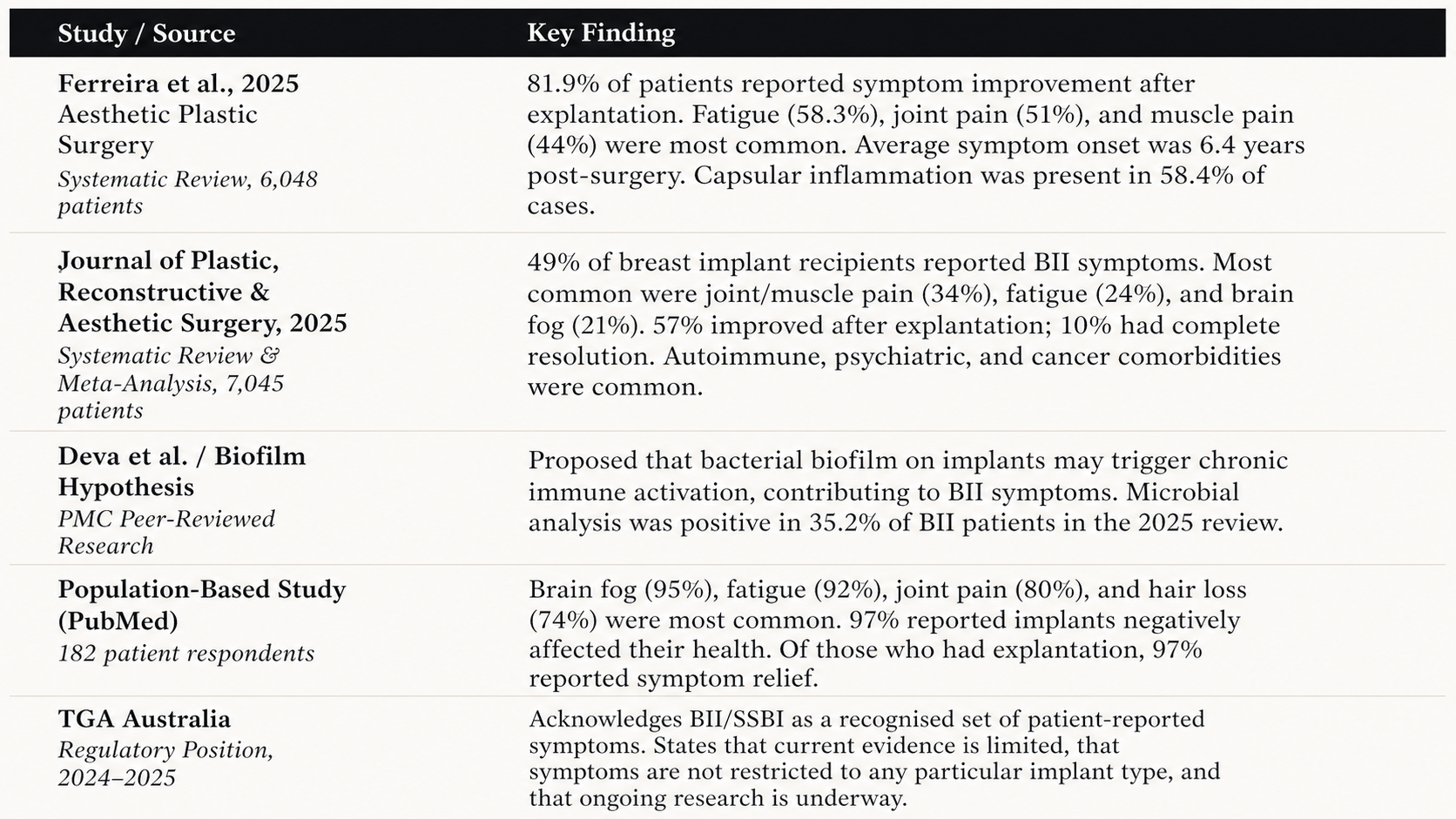
The science on BII has advanced significantly in recent years, moving from dismissal to serious clinical investigation. Here is a summary of the most important current findings:

Does the Type of Implant Matter?
This is one of the most common questions we receive. The TGA's current position is clear: BII symptoms have been reported with all types of breast implants — silicone, saline, smooth, textured, and teardrop — regardless of whether they are ruptured, leaking, or intact.
This means there is currently no evidence that switching from silicone to saline, or from textured to smooth, will necessarily prevent BII. However, the picture is nuanced. Some research points to the role of bacterial biofilms on implant surfaces, and implant surface characteristics may influence this risk — but this remains an area of active investigation.
It's important not to confuse BII with BIA-ALCL (Breast Implant-Associated Anaplastic Large Cell Lymphoma), which is a distinct and separately studied condition linked specifically to textured implants. BIA-ALCL is a rare cancer of the immune cells, while BII refers to systemic symptoms — they are different entities with different evidence bases.
What Are the Possible Causes?
Researchers have proposed several non-mutually exclusive mechanisms that may contribute to BII in susceptible women:
1. Immune System Activation
The 2025 meta-analysis found ANA (antinuclear antibody) positivity — a marker of immune system activity — in approximately 24% of BII patients, compared to much lower rates in the general population. This suggests immune dysregulation may play a role in BII for some women, particularly those with pre-existing autoimmune tendencies.
2. Bacterial Biofilm
A compelling hypothesis proposes that bacterial biofilm — a thin layer of bacteria that can adhere to the implant surface — may trigger a low-grade chronic inflammatory response. This would explain why some women don't develop symptoms for years, and why symptoms may improve after implant removal. Microbial analysis was positive in 35.2% of BII patients reviewed in 2025 research.
3. Silicone Immune Sensitisation
The 2025 systematic review noted "a strong link between silicone breast implants and immune activation, with a notable prevalence of autoimmune markers and inflammatory responses in BII patients." It is theorised that silicone particles or gel bleed may stimulate immune reactions in certain individuals — particularly those with a genetic predisposition to autoimmune conditions.
4. Pre-existing Vulnerabilities
Research consistently finds that BII is more likely in women with a personal or family history of autoimmune conditions, fibromyalgia, chronic fatigue, migraines, or irritable bowel syndrome. This does not mean these women should never have implants — but it does mean the pre-operative conversation is especially important.
What Happens After Explantation?
This is arguably the most clinically important question. The evidence is encouraging but not absolute:
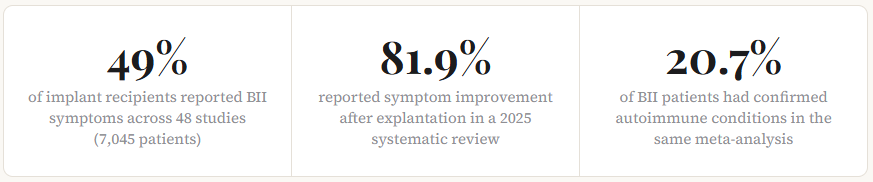
The 2025 meta-analysis found 81.9% of patients reported symptom improvement after explantation. A separate systematic review found 57% improved and 10% achieved complete resolution. A population-based survey found 97% of explanted patients reported some degree of relief.
However, there are important nuances:
Not all patients improve. Symptom improvement is common but not universal. Some women do not experience improvement after removal, particularly if the underlying cause is unrelated to the implants.
The capsule may matter. Some surgeons advocate for total capsulectomy (removal of the fibrous capsule surrounding the implant) alongside explantation, though the evidence for this over simple explantation is not yet definitive.
Timing matters. The longer the period between symptom onset and explantation, the less clear the association between symptoms and the implants themselves — other conditions may have developed in the interim.
Comorbidities must be assessed. Given that autoimmune conditions are present in over 20% of BII patients, appropriate investigation for independent diagnoses should occur alongside any discussion of explantation.
What Does the TGA Say?
Australia's Therapeutic Goods Administration (TGA) operates a dedicated Breast Implant Hub for both consumers and healthcare professionals. Their current position is measured and evolving:
The TGA acknowledges that many women report BII symptoms and that these can significantly impact quality of life. They state that current scientific evidence is limited in establishing whether breast implants directly cause the various symptoms, partly because the symptoms can also be caused by a wide range of unrelated factors.
Importantly, the TGA confirms that symptoms are not restricted to any particular implant type, and that ongoing research is underway. They recommend that women experiencing symptoms similar to those reported for BII discuss them with their surgeon or GP.
Australia's regulatory framework for breast implants is among the most stringent in the world, and the TGA continues active post-market monitoring of all breast implant types.
What Should You Do If You're Concerned?
If you have breast implants and are experiencing symptoms you believe may be related to them, here is a practical framework:
Step 1: Document your symptoms. Keep a diary of what you're experiencing, when symptoms started, and whether they're worsening. Note any patterns (e.g., cyclical symptoms, improvement after rest).
Step 2: See your GP first. Many BII symptoms overlap with thyroid conditions, autoimmune disorders, anaemia, and mood disorders. A thorough GP workup — including blood tests — is important before attributing symptoms to implants.
Step 3: Have an honest conversation with your surgeon. A good cosmetic surgeon will not dismiss your concerns. They should be willing to discuss the evidence, examine you, and refer you appropriately if needed.
Step 4: Consider the full picture before deciding on explantation. Explantation is a surgical procedure with its own risks and recovery. The decision should be made with full information — including an understanding that symptoms may or may not improve after removal.
Step 5: Access credible information. The TGA's Breast Implant Hub is a reliable Australian resource. Be cautious of online communities where confirmation bias and misinformation can distort the picture in both directions.
Frequently Asked Questions
Is breast implant illness recognised in Australia?
Yes, the TGA acknowledges BII — also calling it Systemic Symptoms associated with Breast Implants (SSBI) — and provides information for both consumers and healthcare professionals through its Breast Implant Hub. However, BII does not yet have a formal clinical diagnosis code or universally agreed diagnostic criteria in Australia or internationally.
Can I have breast implants if I have an autoimmune condition?
This requires careful individual assessment. Research shows women with existing autoimmune conditions or a strong family history may have a higher risk of developing BII. This doesn't mean breast augmentation is impossible — it means the pre-operative consultation must include a thorough discussion of personal risk, and the decision must be fully informed.
Will removing my implants cure my BII symptoms?
The majority of women who undergo explantation report symptom improvement — current research suggests around 57–82% experience improvement, with some achieving complete resolution. However, improvement is not guaranteed. Some women's symptoms persist after removal, particularly if other conditions are contributing. The decision to explant should be made carefully, with realistic expectations.
Are saline implants safer than silicone for BII?
According to current evidence, no. The TGA states that BII symptoms have been reported with all types of breast implants — silicone, saline, smooth, textured, and teardrop — regardless of whether they are intact or leaking. There is no current evidence that saline implants carry a lower BII risk than silicone implants.
How long after implant surgery do BII symptoms typically appear?
Research suggests an average onset of approximately 6.4 years after implantation, though symptoms can appear at any time — immediately after surgery or many years later. The wide variability in onset makes it one of the factors that complicates establishing causation.
Is BII the same as BIA-ALCL?
No. These are two entirely different conditions. BIA-ALCL (Breast Implant-Associated Anaplastic Large Cell Lymphoma) is a rare cancer of the immune system linked specifically to textured implants, presenting most often as fluid accumulation around the implant. BII refers to systemic symptoms (fatigue, brain fog, joint pain etc.) and is not a cancer. They require different investigations and management.